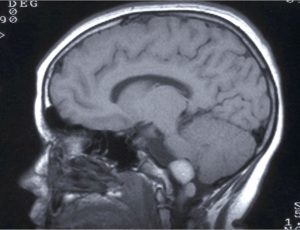
Ependymomas are primary tumours that originate in the ependymal cells, cells that surround ventricular brain cavities and the central canal of the spinal cord. They are included in the group of gliomas.
They represent between 5-10% of neuroepitelial tumours and are especially common among children. 70% of intracranial ependymomas appear in children. They present two peaks of incidence, one at 5 years of age, where they are especially common at a level of the IV ventricle and at 35 when they are more common on a spinal level.
It is the most frequent tumour of the fossa posterior in children, after meduloblastomas and astrocytomas.
 The clinical appearance is common to all other brain tumours, with headache, nausea and vomiting being frequent symptoms of cerebral ependymomas, in many cases due to obstruction of the normal circulation of cerebrospinal fluid (hydrocephalus). In the event de spinal tumours, they may simulate sciatica or clinical deficiency due to spinal compression, paraparesis, tetraparesis in cervical cases, etc.
The clinical appearance is common to all other brain tumours, with headache, nausea and vomiting being frequent symptoms of cerebral ependymomas, in many cases due to obstruction of the normal circulation of cerebrospinal fluid (hydrocephalus). In the event de spinal tumours, they may simulate sciatica or clinical deficiency due to spinal compression, paraparesis, tetraparesis in cervical cases, etc.
The WHO classifies ependymomas in four groups.
- Myxopapillary ependymoma (grade I)
- Subependymoma (grade I)
- Ependymoma (grade II)
- Anaplastic ependymoma (grade III)
The treatment of choice will be surgery in those cases where it is technically possible. Complete resection is especially difficult in tumours of the posterior fossa as many of them originate in the fourth ventricle floor where very important brain nuclei are located and whose damage brings about very important neurological deficits. In cases where they originate in the ceiling of the fourth ventricle resection is possible. In cases of greater malignancy (grade II-III) treatment may be associated with radiotherapy or chemotherapy. They are especially radiosensitive tumours.
The prognosis seems more related to the degree of resection rather than the histological grade.
Leptomeningeal dissemination (through the CSF) is especially common in cases of anaplastic ependymomas although it may also occur in ependymoma (grade II) or myxopapillary (grade I), and so after diagnosis of this tumour lineage the whole neural axis should be closely examined.