Oligodendrogliomas (ODG) form part of the glioma group. They are primary brain tumours, that is, tumours that originate from the cells that form the normal brain structure, the oligodendrocytes.
 They represent about 3-4% of all brain tumours, presenting a peak incidence between 35-55 years of age, and being most frequent in males with a ratio of 3:2.
They represent about 3-4% of all brain tumours, presenting a peak incidence between 35-55 years of age, and being most frequent in males with a ratio of 3:2.
The clinical signs are similar to other brain tumours, headache, neurological deficits, etc., even though these tumours are known for causing epileptic seizures.
Diagnosis is based on imaging, CT or MRI. This type of tumour has two main characteristics, the presence de intra-tumoural calcification and the predilection for the frontal lobe. Confirmation of the diagnosis will correspond to anatomic pathologic analysis, the “fried egg-like cells” are a good indication of the diagnosis.
Although they may be located at any point of the neural axis, location on a medullary level is exceptional and only represents about 4% of all medullary tumours.
About 40% of all oligodendrogliomas have components from other glial, astrocytary or ependymal lines, and in these cases are called oligoastrocytomas or mixed gliomas. Pure ODG appear to have a better prognosis than mixed ones and these, in turn, a better prognosis than pure astrocytomas.
Many classifications have been developed for the different types of oligodendrogliomas, many of them now abandoned as they had no prognostic value. Currently the WHO classifies ODG as an atypical oligodendroglioma, corresponding to grade II and anaplastic oligodendroglioma, corresponding to grade III if a parallelism is established with astrocytomas.
Over the last few years genetic studies have appeared that aid in predicting tumoural response to certain treatments, in reference to ODG the presence of 1p19q deletion predicts a favourable response to chemotherapy.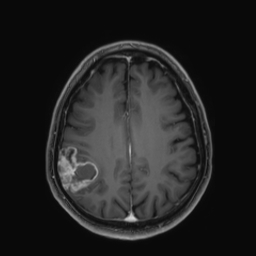
The treatment of choice will be surgical resection in those cases where it is technically possible. The location of the tumour: the general condition of the patient and their age will be factors to be assessed when establishing this indication.
The fact that they are heterogeneous tumours, and that there is no unanimous agreement on the need to offer radiotherapeutic treatment to these patients and which is the best chemotherapy regime, have brought about the appearance of a multitude of treatment protocols for these tumours, especially in reference to chemotherapy and radiotherapy.